Corns, also referred to as clavi, are painful, hyperkeratotic papules of the skin that develop in response to excess pressure on the bony prominences of the feet and toes. Corns are often seen in athletes and in patient populations exposed to uneven friction from footwear or gait abnormalities, including elderly persons, diabetic patients, and amputees. Abnormal foot mechanics, foot deformities, high activity level, and more serious conditions such as peripheral neuropathy also contribute to the formation of corns.[1] Corns are associated with considerable morbidity secondary to pain; fortunately, many treatment and preventative options are available that provide a high rate of mitigation.
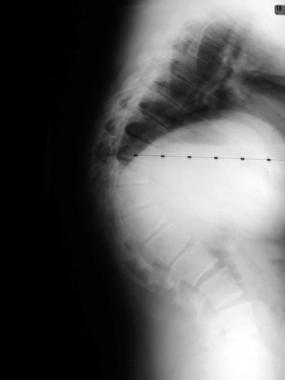
Clinically, 3 types of corns have been described. The first is a hard corn, or heloma durum, notable for its dry, horny appearance. It is found most commonly over the interphalangeal joints. The second is a soft corn, or heloma molle, described as such because of its macerated texture secondary to moisture. It is generally found in interdigital locations.[2, 3] The third type is a periungual corn, and this type occurs near or on the edge of a nail.[4] Note the image below.
 Hard corn over the proximal interphalangeal joint of second toe. Courtesy of James K. DeOrio, MD.
Hard corn over the proximal interphalangeal joint of second toe. Courtesy of James K. DeOrio, MD.
Corns are often misdiagnosed as calluses, which are also hyperkeratotic skin lesions resulting from excess friction. However, calluses develop from forces distributed over a broad area of skin, whereas corns develop from more localized forces.[5] Calluses are often considered desirable for some activities (eg, gymnastics, weightlifting), and they lack a central core, which is characteristically revealed in corns upon removal of the upper hyperkeratotic layer of skin. Corns can occur within an area of callus,[6] such as on the plantar surface. Note the image below.
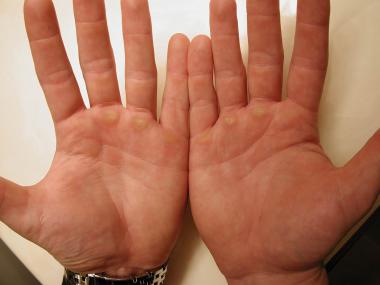 Calluses on the palmar surface of the hands of a body builder. Courtesy of James K. DeOrio, MD.
Next
Calluses on the palmar surface of the hands of a body builder. Courtesy of James K. DeOrio, MD.
Next
Corns are the result of mechanical trauma to the skin culminating in hyperplasia of the epidermis. Most commonly, friction and pressure between the bones of the foot and ill-fitting footwear cause a normal physiological response—proliferation of the stratum corneum. One of the primary roles of the stratum corneum is to provide a barrier to mechanical injury. Any insult compromising this barrier causes homeostatic changes and the release of cytokines into the epidermis, stimulating an increase in synthesis of the stratum corneum. When the insult is chronic and the mechanical defect is not repaired, hyperplasia and inflammation are common.[7] With corns, external mechanical forces are focused on a localized area of the skin, ultimately leading to impaction of the stratum corneum and the formation of a hard keratin plug that presses painfully into the papillary dermis, which is known as a radix or nucleus.[3, 5]
A callus is a local thickening of skin, characterized by accelerated keratinization and a reduced rate of desquamation. Expression of cornification-related molecules, including involucrin, filaggrin, caspase 14, and calcium-sensing receptor, are higher in the anterior aspect of the heel. Expression of adhesive proteins such as corneodesmosin, desmoglein 1, and desmocollin 1 are also increased in the heel. Protease-activated receptor 2 expression is reduced in the stratum granulosum in the heel. The number of proliferating cells in the stratum basale is significantly increased in the heel compared with other areas of the foot. Therefore, calluses are proposed to form as a result of hyperproliferation and incomplete differentiation of epidermal keratinocytes and increased expression of adhesion molecules.[8]
United States
Corns are one of the most common foot conditions in the United States, particularly amongst older patients.
International
Corns are common worldwide. Any weight-bearing human is susceptible to the development of corns.
The most common symptoms associated with corns are pain upon ambulation and restriction of activity secondary to pain. Corns are generally not associated with mortality; however, recognizing the potential for a maltreated corn, soft corns in particular, to develop into a life-threatening secondary infection (bacterial or fungal) is important in patients with diabetes mellitus or immunosuppression.
See Diabetes Mellitus, Type 1; Diabetes Mellitus, Type 2; and Diabetic Foot Infections for follow-up information.
An epidemiological study evaluating the prevalence of foot conditions amongst a diverse sample of adults from the northeastern United States revealed a significant difference in rates of corns amongst ethnic groups. African Americans had a significantly higher rate of corns and calluses compared with non-Hispanic white and Puerto Rican participants (70% vs 58% vs 34.1%).[9]
Amongst elderly populations, both men and women have been reported to wear shoes too narrow for their feet. Women have been reported to wear shoes that are also shorter than their feet. Both narrow and short footwear can lead to the development of corns, in addition to foot deformities.[10]
Hyperkeratotic lesions of the foot (including corns and calluses) have been reported to affect 20-65% of people aged 65 or older.[9, 11, 12]
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved