Patients with inflammatory types of arthritis such as rheumatoid arthritis and psoriatic arthritis often have shoulder problems. However, more often than not, a patient presenting with shoulder pain to the rheumatologist will have another reason besides the arthritis for the discomfort they are feeling.
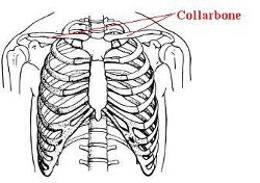
The shoulder is a complicated and complex joint consisting of the interaction of two major bones forming the glenohumeral joint- the joint that joins the upper arm bone to the shoulder blade. The acromioclavicular joint which joins the clavicle (collarbone) to the shoulder blade is also part of this complex. The muscles that help move the shoulder consist primarily of the rotator cuff muscles and their associated tendons: supraspinatus, infraspinatus, subscapularis, and teres minor.
The biceps muscle and tendon are also responsible for shoulder movement as is the deltoid muscle. The shoulder complex is held together via a complicated network of ligaments and tendons that allow the shoulder to have the widest range of motion of any joint in the body. The shoulder complex is surrounded by small fluid filled sacs, called bursae that help to cushion the shoulder joint and allow more purposeful gliding motions of the joint.
Shoulder pain is responsible for about 16% of all complaints having to do with muscles or joints. Shoulder pain becomes defined as being chronic if it lasts 6 months or longer. Age is a general predictor of cause. In patients younger than 40 years, shoulder instability and mild rotator cuff disease are more common. Older patients usually have conditions such as adhesive capsulitis (frozen shoulder), osteoarthritis, and more advanced rotator cuff problems.
Pain located at the top and front of the shoulder is usually due to problems related to the AC (acromioclavicular) joint - that is, the joint that joins the collarbone to the shoulder blade.
By contrast, pain involving the outside of the upper arm near the shoulder joint is often due to bursitis involving the bursa located beneath the deltoid muscle or to tendonitis affecting the rotator cuff.
A diagnosis starts with the history. During the history, the physician will inquire as to the location and duration of pain, whether the pain is present at night, and what types of body positions and movements aggravate the pain.
In addition the range of motion of the shoulder will be assessed. There are two methods for measuring range of motion. Active range of motion is the range of motion a patient can perform on their own. Passive range of motion is what the patient can do with the assistance of the physician.
Problems like tendonitis and bursitis will show that a patient has limited active range of motion but relatively normal passive range of motion.
Loss of both active and passive range of motion suggests adhesive capsulitis or glenohumeral arthritis (arthritis affecting the joint that joins the humerus [upper arm bone] to the scapula [shoulder blade]).
Certain maneuvers designed to pinch" the rotator cuff against the acromion (the outside part of the shoulder blade) can reproduce the pain in some patients. This condition is called impingement.
Imaging procedures such as x-ray may be helpful in some instances. For example, it can show calcium deposits in tendons or show severe arthritis in the AC joint.
The preferred imaging procedure for suspected rotator cuff disorders is MRI; however, ultrasound is becoming more popular as a cost-effective alternative to MRI. Some studies have indicated that diagnostic ultrasound is actually more precise than MRI for detecting rotator cuff tears.
Conservative treatment is usually initiated for most patients with chronic shoulder pain. This treatment should consist of modification of daily activities such as reduction of overhead activity in patients with rotator cuff disease, glenohumeral osteoarthritis, or adhesive capsulitis.
Cross-body shoulder movements such as swinging a baseball bat, tennis racket or golf club should be limited among patients with AC arthritis.
Non-steroidal anti-inflammatory drugs are frequently used and can be effective.
Injections of glucocorticoids (cortisone") into the space beneath the acromion are also useful for reducing inflammation. Injections of glucocorticoids directly into the glenohumeral joint are effective in reducing pain and increasing function among patients with adhesive capsulitis. These injections need to be guided using either ultrasound or fluoroscopy to be effective.
Adhesive capsulitis should be treated with a combination of steroid injections as well as physical therapy. Referral to an orthopedist for either manipulation of the shoulder under general anesthesia or arthroscopy is recommended for patients with adhesive capsulitis who do not respond to 2-3 months of therapy.
Osteoarthritis of the glenohumeral joint may respond to NSAIDS and injections into the glenohumeral joint. Physical therapy may also be useful but it should be done gently since too vigorous therapy can aggravate this condition.
Patients with acute massive rotator cuff tears are fairly easy to diagnose and should be referred to an orthopedist as quickly as possible to ensure a good surgical outcome. Massive tears that have been present for 6 weeks or longer are often difficult to repair.
Patients with small tears of the rotator cuff often respond to conservative treatment.
Newer techniques involving the use of tenodesis (irritating" the tendon to stimulate bleeding) followed by ultrasound guided injection of platelet rich plasma to help with the healing process may allow patients with rotator cuff tears to avoid surgery. This same procedure is being evaluated for arthritis processes as well.
Patients with rotator cuff tears not responding to more conservative measures can be referred to an orthopedist.