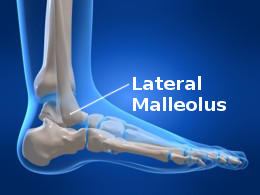
Because of the large number of locations where fractures occurs and the different bones involved there is a variety of plates available. The dynamic compression plate or DCP allows a sliding technique to be used because of the screw holes being angled away from a central point. Once the screws are inserted and tightened they apply an inwards compression force, bringing the fragments into stronger contact. The ulna and the ankle lateral malleolus are fixed with thin plates of about one mm in thickness which can be shaped to the area required. Fractures close to a joint need specially designed plates to facilitate fixation and reduce impingement.
Fractures of the upper femur are fixed by using plates with a 95 degree angle so that the mechanical axis of the upper femur can be restored at this angle. Inserting this kind of fixation requires that the surgeon thinks in three dimensions as are all must be correctly aligned to restore normal anatomy. Reconstruction plates are less thick than dynamic compression plates and can be contoured in three dimensions for the acetabulum and pelvis. Fractures close to or next to prostheses such as hip replacements or knee replacements are fixed with larger plates with the addition of cerclage wires.
Strong fragment compression and close anatomical restoration of normal alignment can lead to a very stable fixation and if this is produced by the fixation then primary healing will be the main healing process. There is dead bone close to the fracture site and this is absorbed by bone absorbing cells known as osteoclasts, after which blood vessels grow in along with bone producing cells known as osteoblasts. Osteoporosis under a plate can occur from the interruption in blood supply which can be produced by the fixation. Once the plate is removed the bone is less strong and along with the screw holes this means care needs to be taken in physiotherapy for the patient because of this.
Internal fixation with a plate involves opening up the fracture site and removing the blood clot, reducing the fragments to an anatomically acceptable alignment. A fracture interrupts the blood supply across and around a fracture and the remaining blood supply is provided by the periosteal bone lining. The periosteum should be preserved and not stripped away during the operation or healing could be delayed from reduced vascular supply. Unstable comminuted fractures are more difficult to fix and bridge plates are used to fix the two main parts and keep the important aspects of the bone in line, the rotation, alignment and length of the bones. However this form of weaker fixation cannot tolerate any significant level of load.
The Less Invasive Surgical Stabilisation plating system (LISS) is a modern fixation system which limits the contact between the metal and the bone, lowering the risks of the blood supply in the damaged area becoming compromised. These designs are more mouldable to the bony contours and have the ability to apply locking screws, allowing these designs to keep the desired bony alignment whilst simultaneously managing to resist significant forces during the period of healing. Choice of these newer designs is indicated in managing fractures of the end of bones such as the radius, humerus and femur.
Conventional plating techniques are adequate to fix fractures where access to the areas is easy and in cases where the fractures are of a stable type, incorporating fractures of bony shafts such as the ulna, humerus and radius. With osteoporotic bone and difficult fixation options the locking systems will be more appropriate. As they are much more expensive than the conventional systems they are not yet the default choice in all cases but look likely to be more widely used as the cost comes down. They may well be cost effective if cases of malunion which require revision are taken into account.
Nails
It was in the 1930s that Kuntscher refined the intramedullary nailing technique which then became the treatment of choice for shaft fractures of the femur. Humeral and tibial fractures as well as femoral breaks nearer the bone ends were the next progression. Early joint movement and weight bearing walking is allowed by this.