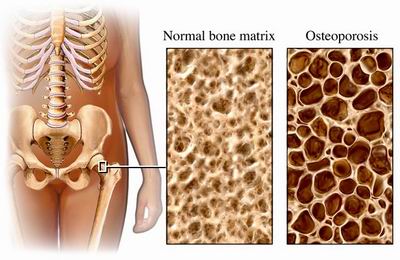
Back and neck pain is one of the leading causes of lost work time, second only to the common cold. It affects 65-85% of the population of the United States at some point in their lives. The most common cause is sprain, strain, or spasm usually brought on by poor lifting techniques, improper posture, or an unhealthy ergonomic environment. Another common cause is disc problems brought on by injury, wear and tear, or age. Other causes include spinal stenosis (spinal sten-oh-sis), osteoarthritis (os-t-o-arth-rye-tis), osteoporosis (os-t-o-pour-o-sis), and other conditions.
Pain management often takes a multidisciplinary approach to minimize or eliminate pain. The goals include increasing physical activity, eliminating unsafe medication use, and learning lifestyle behaviors that work toward wellness. The purpose of this chapter is to help you to understand pain management. Included is an explanation of the different types of pain and treatments pain management specialists use to fight pain.
Also, you may take a Chronic Pain Treatments Quiz to test your knowledge and learn about the most effective ways to treat chronic back and neck pain.
• Types of Back and Neck Pain
Acute Pain (ah-cute pain) can be defined as severe short-term pain. Post-operative pain is an example. Acute pain is self-limiting, which means the pain acts to warn you to cease or limit activity that could cause additional tissue damage. The more intense and prolonged an acute pain episode is, the more likely it will lead to chronic pain. This makes sense given the information that we are beginning to learn about how the central nervous system changes in response to intense pain. As a result of intense pain, neurons in the spinal cord that help to prevent pain transmissions actually die. At the same time, pain-transmitting neurons grow more connections to other nerves, become more sensitive, and react more strongly to painful stimulus.
The study of neuroplasticity (nu-row-plaz-te-city), or how the nervous system changes and molds itself, is one of the hottest new areas in neuroscience. It seems to be the basis for the processes of learning and memory. It appears however, that the nervous system not only learns useful information but also 'learns' or remembers pain leading to the development of chronic pain.
Chronic Pain. Rather than being the symptom of a disease process, chronic pain is itself a disease process. Chronic pain is unrelenting and not self-limiting. It can persist for years and even decades after the initial injury. There are many factors that affect the development of chronic pain such as age, level of disability, depression, or the presence of nerve damage.
Neuropathic Pain (nu-row-path-eck pain) is usually described by patients as burning, electric, tingling, and shooting in nature. Often this type of pain cannot be controlled using traditional pain killing oral drugs. Management of neuropathic pain may include other medications (that are often not thought of as pain medicines) and multiple treatment modalities such as physical therapy, physical rehabilitation, relaxation training, trigger point injections, epidural steroid injections, sympathetic blocks, spinal cord stimulators, intrathecal morphine pump systems, and various surgical techniques.
Nociceptive Pain (no-si-sep-tive pain) is localized pain, which is usually described by patients as sharp, aching, or throbbing. Post-operative pain, pain associated with trauma, and arthritic pain are examples of nociceptive pain. Nociceptive pain usually responds to non-steroidal anti-inflammatory drugs (NSAIDs) and opioids (oh-pe-oids, strong prescription pain killers).
• Pain Management Treatments and Therapies
Anti-Depressant Medications. There is considerable evidence that tricyclic anti-depressants are effective for the treatment of a variety of pain conditions such as migraine headache and neuropathic pain.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) are valuable analgesics (pain relieving medications). These drugs do not alter the patient's cognitive functions, cause respiratory depression, or nausea. However, NSAIDs are associated with significant side effects especially with long-term use.
Epidural Steroid Injections (ESI). The traditional epidural (ep-e-do-ral) steroid injection technique involves the physician feeling the patient's spine in order to guide the placement of the needle between the spinal vertebrae. A newer technique involves using x-ray fluoroscopy to guide the needle directly into the neural foramen; the point where the affected nerve root exits the spinal canal.
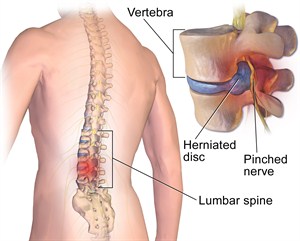
Injections of steroids into the lumbar epidural space are particularly useful to alleviate pain that radiates from the lower back into a leg. This pain may be caused by disc herniation or spinal stenosis, which triggers nerve root irritation, inflammation, and pain. Similarly, ESIs are used to treat neck pain that extends into the arms.
Facet Joint Injections involve the injection of steroid medication into the affected spinal facet joint (fah-set joint) to reduce inflammation and pain. Injections into these joints or blocks of the nerves that feed the facet joints can often be very helpful to relieve pain. This problem is more common in the lumbar spine, but does occur in the cervical spine too.
Trigger Point Injections are muscle blocks. Muscles chronically tense or in spasm become tender and painful. The pain triggers more spasm that can develop into a vicious cycle. Injections into the muscle can help to break the cycle.
Nerve Blocks are injections of medication onto or near nerves. The medications that are injected include local anesthetics, steroids, and opioids. Blocks are used to control acute pain (e.g. shot at the dentist or an epidural block for the surgical delivery of a baby). X-ray fluoroscopic guidance is sometimes used for accurate needle placement. Blocks can provide periods of dramatic pain relief, which promotes the desensitization of sensory pathways. Steroids can help reduce nerve and joint inflammation, and the abnormal triggering of signals from injured nerves. Further, blocks are used to provide diagnostic information such as helping to determine the pain source.
Peripheral Nerve Blocks affect the peripheral nerves; nerves beyond the brain and spinal cord. These nerves transmit sensation and motor (movement) signals.
Sympathetic Nerve Blocks. Chronic pain conditions often involve sympathetic nerve malfunctions. These nerves regulate blood flow, sweating, and glandular function. For example, blocks administered in different areas of the spine help to reduce pain that involves the face, arm, hands, legs, and feet.
Physical Therapy (PT) addresses body mechanics (posture), building strength and flexibility through exercise, injury prevention, and utilizes many modalities. Modalities include electrical stimulation, heat and ice therapy, hydrotherapy, ultrasound, and massage.
Biofeedback is used to treat many types of conditions including chronic pain, migraine headache, spinal cord injury, and movement disorders. It is a type of relaxation training and behavior modification. Biofeedback works to control physiological reactions such as muscle tension, body temperature, heart rate, brain wave activity, and other life responses. The therapy requires the patient's intense participation to learn how to control these functions. Biofeedback does not work for all patients. Electrical sensors, attached to monitoring equipment, are applied to special points on the patient's body. The monitoring equipment feeds back the patient's progress. The biofeedback therapist teaches the patient mental and physical exercises, visualization, and deep breathing to treat their specific disorder (e.g. low back muscle spasms).
This article is an excerpt from Dr. Stewart G. Eidelson's book, Advanced Technologies to Treat Neck and Back Pain, A Patient's Guide (March 2005).
To learn about Dr. Richeimer’s practice, click here.
Copyright © www.orthopaedics.win Bone Health All Rights Reserved