Isthmic spondylolisthesis should be differentiated from degenerative spondylolisthesis. Degenerative spondylolisthesis occurs due to the aging process along with the development of marked facet joint arthritis with rotatory vertebral slip. Degenerative spondylolisthesis occurs mostly at the L4-L5 (fourth and fifth lumbar vertebrae) level as opposed to its isthmic counterpart, which occurs most often at the lumbosacral level (L5-S1).
Although in most instances spondylolisthesis develops before adulthood, only 25% of children and adolescents experience symptoms such as back pain and/or buttock and thigh pain, especially in patients with a high-grade slip. Many adults are unaware of their spondylolisthesis until it becomes symptomatic. Symptoms usually begin to occur between the ages of 30 and 50 years. This raises an interesting question:
If spondylolisthesis is a developmental condition that occurs in late childhood or adolescence and seldom after the age of 20, why is it clinically silent in so many adults until midlife?
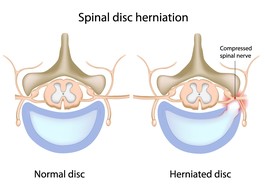
The lumbosacral joint is subjected to considerable anterior-directed shear forces. The paired facet joints, pars interarticularis, and intervertebral disc are the main anatomical structures that resist these forces. In the presence of spondylolysis, with or without mild spondylolisthesis, the facet joints become unable to resist the anterior shear forces.
In the presence of spondylolysis, the intervertebral disc is the main structure that retains the stability of the segment. As long as the disc is capable of maintaining its biomechanical and biochemical integrity, mild spondylolisthesis will be stable, despite the presence of a mild slip and the loss of resistance to shear forces provided by the posterior vertebral structures. Once the disc degenerates, the main source of stability is lost and the vertebral slip increases, leading to symptoms of back and leg pain.
Copyright © www.orthopaedics.win Bone Health All Rights Reserved